
In the Interfaith America Podcast episode featuring David Brooks, Eboo Patel drops a MacIntyre quote: “I cannot tell you who I am or what I am to do if I do not tell you the story or stories that I am a part of.” This sparked a poignant conversation for a group of women in healthcare on a recent Saturday in a Philz Coffee shop in Sacramento, thanks to Interfaith America’s Podcast Engagement Award.
As healthcare workers, we willingly leave at the hospital door our religious, faith, or spiritual identities so we can meet patients wherever they are at. In an effort to be unbiased towards the diverse populations that fill our beds, much like an actor or actress in a play, we take on a neutral and hopefully, welcoming, presence to hold whatever journey the patient is on.
Engagement Award
Receive funding for your own intentional reflection or for hosting conversations about the podcast.
I see the benefit of this choice, I understand it on a rational level, but I cannot help but wonder, what is lost? What is lost when we shape shift ourselves daily to fit a system bent on efficiency and checklists? Is there a way to be in touch with our specific religious and spiritual traditions, but still meet the vulnerable where they are at?
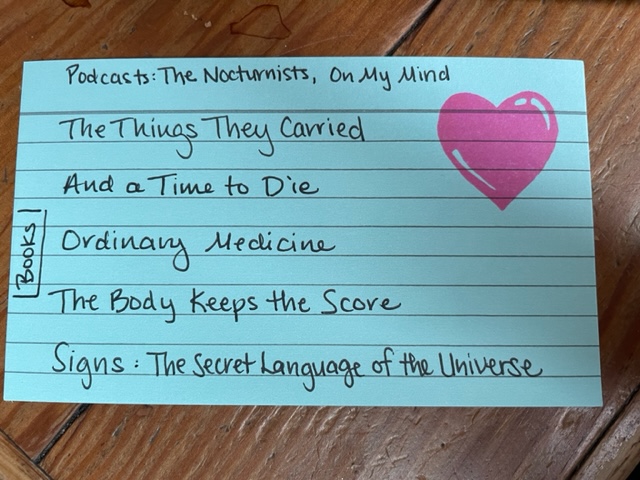
Having a dedicated space to explore these sorts of questions with other women in healthcare, was like floodgates, opened. Stories of who and what shaped us couldn’t come out fast enough. Whom we wish to honor our work with, the complicated relationships we have with the religions of our upbringings, and the things we cannot shed, try as we might. For myself, I cannot break the habit of studying the Bible in community with others that was given to me by an evangelical organization, over a decade ago. Although no longer part of an evangelical organization, this practice undeniably buoys me and grounds me, week to week. It helps build my resilience to navigate the inherent suffering we have chosen to witness as healthcare workers.
“I cannot tell you who I am or what I am to do if I do not tell you the story or stories that I am a part of.”
Eboo mentioned the majority of Americans do not attend a religious service and he worries about the loss of community and resilience we see as people step away from religion. As co-founder of a social venture building reflective spaces for women in healthcare, I sharply recognize the need and value of such spaces, and hope our interfaith, reflective spaces can be a part of rebuilding communities of belonging for healthcare workers who don’t quite fit somewhere else. Another participant agrees but adds the perspective of her patients. She notices they are lonely and wishes she could prescribe communities of belonging to her patients. For example, there is ample research to support that those with supportive communities have better health outcomes, such as better breast cancer survival.
Furthermore, religious communities can be an important compass in healthcare decision making. We discussed the implications of guidelines created by governing bodies that do not take into account the fact that many patients would choose quality of life over the quantity of life we often default to in healthcare decision making. For example, the guideline that recommends placement an automatic implanted defibrillator in heart failure patients. This is specifically problematic for patients over 80 years old. We technically save their life by prolonging it but take away the chance of swift death that many say they desire. These guidelines are often more shaped by Medicare reimbursement criteria than meaningful, spiritually-informed conversations around death and dying. This brings us to wonder what is medicine’s goal in an aging society? Who gets to decide and how? If our patients are less and less a part of a regular religious community, but healthcare has offloaded conversations of death and dying to patients and their family, how are we to prepare or make sense of the final transition?
As you can see, we don’t need much to get going, and were left with perhaps more questions than answers. Discussing the role of religious identity and community for both patient and provider showed us the need for both to have spaces of connection and meaning making.
I believe our conversation was so overflowing with ideas, due to the fact that we are usually going too fast to get the privilege to stop and ask these sorts of questions about our own experiences in the clinical setting. As a result, we are thankful to Interfaith America to offer us the precious time and space to host these much needed discussions to help us make meaning of our own stories and work and to join the conversation already in progress.
Although many of us had just met for the first time, we were fast friends. Bounded by our desire for connection and processing of our own difficulties as healthcare workers, everyone eagerly agreed to meet again at our next event, an Introspective Spaces in-person retreat on April 22. I am thankful we will continue these conversations in a longer format, as well as explore contemplative and reflective practices to ground us for the work of reimagining healthcare ahead.

Laura Holford, RN MSN, is an oncology certified nurse, nursing educator, and community health nurse committed to working to reduce nursing burnout and moral distress as Co-Founder of Introspective Spaces.
Like many mystics before her, she believes that contemplation and action cannot be separated and finds herself naturally helping others build reflective, imaginative, and spiritual practices to ground their action and work in the world.




{kind=link}
{kind=link}
{kind=link}